Cerebral Aneurysm: Rupture Risk and Treatment Options
A cerebral aneurysm isn’t something you hear about often-until it’s too late. It’s a weak spot in a brain artery that balloons out like a tiny balloon, and if it bursts, it can cause a deadly bleed in the space around the brain. This isn’t rare. About 3.2% of people worldwide have one, often without knowing. Most never rupture. But for those who do, the odds are brutal: 30-40% die within the first 24 hours. The good news? We now know a lot more about what makes an aneurysm dangerous-and what to do about it.
What Makes an Aneurysm Likely to Burst?
Not all aneurysms are created equal. Size matters, but it’s not the whole story. An aneurysm that’s 7 mm or larger has over 3 times higher risk of rupturing than smaller ones. But even a tiny one can burst if it’s in the wrong place. Aneurysms at the anterior communicating artery (AComm) are especially risky-even if they’re under 5 mm. These spots carry 2.4 times higher rupture risk than others.
Shape is another big clue. Aneurysms with irregular shapes, or those with a smaller bulge sticking off the main sac (called a daughter sac), are 68% more likely to rupture than smooth, round ones. Blood flow plays a role too. Areas where blood swirls or flows slowly create stress on the artery wall. Studies show 83% of ruptured aneurysms had abnormal flow patterns, compared to just 42% of unruptured ones.
Then there are the things you can’t change. Age is a major factor. People over 65 have a 2.7-fold higher risk than younger adults. Women are more likely to have them than men-1.6 times more. And if two or more close family members had one, your risk jumps fourfold.
But here’s the part you can control: lifestyle. Smoking is the biggest modifiable risk. Current smokers have a 3.1-fold higher risk than non-smokers. If you smoke more than 10 cigarettes a day, your risk goes up another 47%. High blood pressure is just as dangerous. Systolic pressure above 140 mmHg triples the chance of rupture. Heavy drinking-more than 14 drinks a week-adds another 32% risk.
The PHASES Score: A Real-World Tool for Deciding What to Do
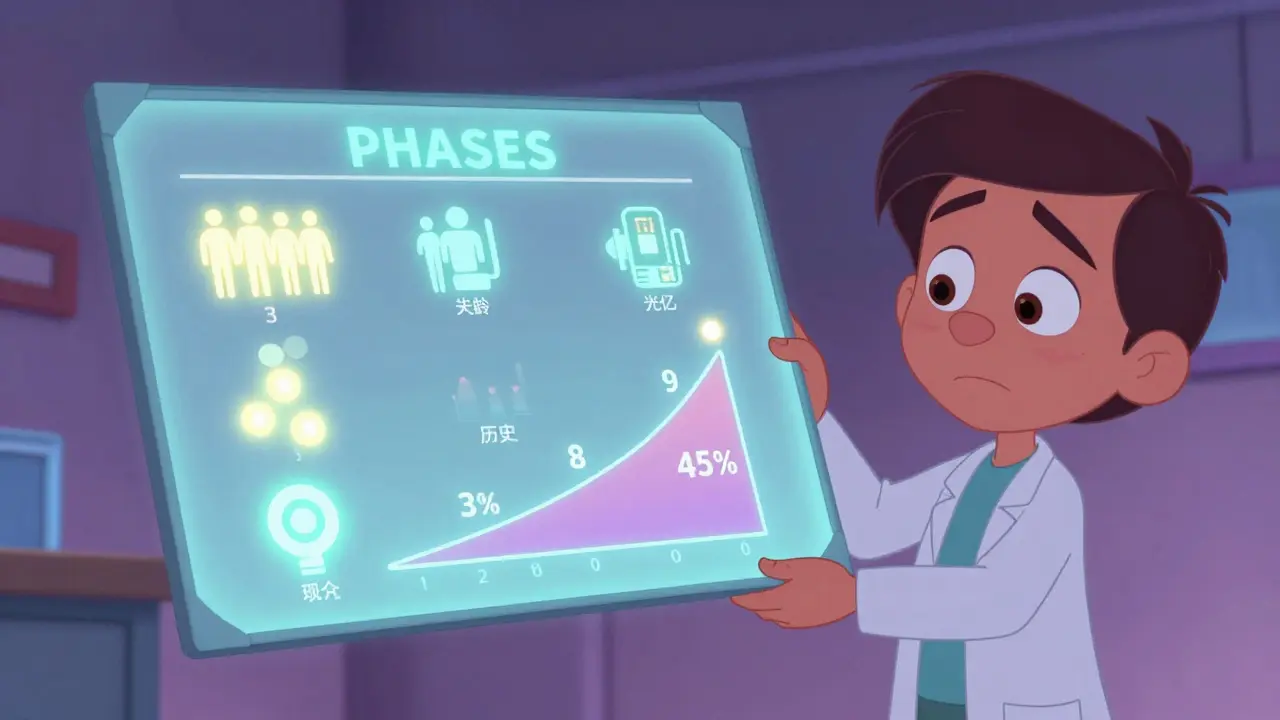
Doctors don’t just guess whether to treat an aneurysm. They use tools. The PHASES score is one of the most trusted. It combines six factors: your population (where you live), blood pressure, age, aneurysm size, whether you’ve had a previous bleed, and where the aneurysm is located. Each factor gets a point. Add them up.
A score of 0-3 means your 5-year rupture risk is only 3%. That’s low enough that monitoring is usually the best choice. A score of 9-10? Your risk jumps to 45%. That’s when treatment is strongly recommended.
Each extra point in the PHASES score increases your risk by 32%. So if your score goes from 4 to 5, your chance of rupture in five years climbs noticeably. This isn’t just theory-it’s based on data from over 3,270 patients across six major studies. It’s why doctors now use it to guide decisions for thousands every year.
Treatment Options: Clipping, Coiling, and Flow Diversion
If treatment is needed, there are three main options. Each has pros and cons.
Microsurgical clipping is the oldest method. A neurosurgeon opens the skull, finds the aneurysm, and places a tiny titanium clip across its neck. It’s like shutting off a leak at the source. Success rates are high-95% of aneurysms are fully blocked. Long-term cure rates? 88-92%. But it’s invasive. Recovery takes weeks. And for patients over 70, complication rates jump by 35%.
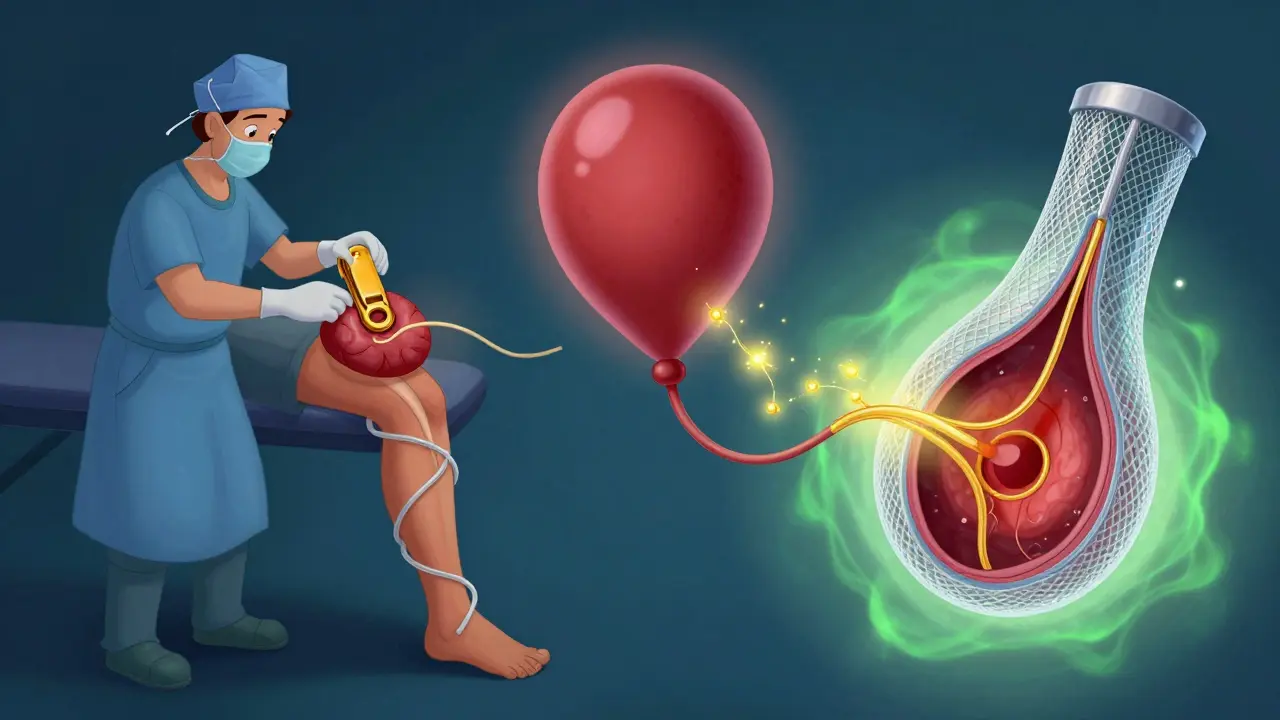
Endovascular coiling is less invasive. A catheter is threaded from the groin up to the brain. Tiny platinum coils are packed into the aneurysm, triggering a blood clot that seals it off. At six months, 78-85% are completely blocked. It’s faster, less painful, and has lower short-term death rates. The famous ISAT trial showed coiling cut 1-year mortality by 22.6% compared to clipping (8.1% vs 10.1%). But it’s not perfect. About 15.7% of coiled aneurysms need retreatment over 12 years-much higher than clipping’s 6.2%.
Flow diversion is the newest option. Instead of filling the aneurysm, it redirects blood flow away from it using a special mesh stent. The idea? Let the aneurysm slowly shrink and scar over. The Pipeline Embolization Device and newer versions like PED-PLATINIUM show 85.5% complete occlusion at one year. It’s especially useful for large, wide-necked, or complex aneurysms. But it takes time-sometimes over a year-for full healing. And it requires long-term blood thinners, which can be risky for some.
Who Gets Which Treatment?
There’s no one-size-fits-all. Your choice depends on several things:
- Size and shape: Aneurysms over 7 mm, irregular, or with daughter sacs usually get treated. Flow diversion works best for wide-necked ones (>4 mm).
- Location: Aneurysms in the back of the brain (posterior circulation) are harder to clip safely. They have a 22% higher complication rate with surgery, so coiling or flow diversion are often preferred.
- Your age and health: If you’re over 70 or have other serious conditions like heart disease or uncontrolled high blood pressure, surgery becomes riskier. Coiling or flow diversion may be safer.
- Previous rupture: If you’ve already had one rupture, your chance of another is 5.2 times higher. Treatment is almost always recommended.
- Multiple aneurysms: Having more than one increases rupture risk by 3.8 times. Doctors usually treat the most dangerous one first.
There’s also a new option for tricky aneurysms at branch points in the artery-the WEB (Woven EndoBridge) device. Approved in 2019, it’s shaped like a tiny mesh sphere. In trials, it achieved 71.4% complete occlusion at one year. It’s changing how we treat some of the most stubborn cases.
What About Not Treating It?
Many small aneurysms are never treated. The UCAS Japan study found that aneurysms under 5 mm in the front of the brain had only a 0.2% chance of rupturing over five years. In the back? Just 0.7%. For these, watching and waiting-with annual MRA scans-is often the best plan.
But you can’t just ignore it. Medical management is key. Lowering blood pressure to under 130/80 mmHg cuts rupture risk significantly. Quitting smoking reduces your risk by 54% within two years. Cutting back on alcohol helps too. These aren’t just suggestions-they’re proven ways to stay safe.
What’s Next? The Future of Prediction and Treatment
Science is moving fast. Researchers are now looking at genetic markers. The HUNT study found 17 gene locations linked to aneurysm formation and rupture. In the future, a simple blood test might tell you if you’re at high genetic risk.
Machine learning is also stepping in. Instead of relying on just size or shape, new models analyze 42 different factors-blood flow patterns, wall thickness, even tiny changes over time. One model had a C-index of 0.72, meaning it’s pretty good at predicting who’s most at risk. These tools could soon replace older scoring systems.
One thing is clear: we’re getting better at spotting danger before it happens. And that’s saving lives.
So let me get this straight - we’ve got a ticking time bomb in half a percent of the population and the only thing stopping it is whether you smoked your last cigarette or not? I mean, if you’re over 65, female, have a 6mm aneurysm near the AComm, and your BP is 145... congrats, you’re basically playing Russian roulette with your brain. And the doctors just hand you a PHASES score like it’s a weather forecast. 3% risk? Sure. Until it’s not. Then it’s 100%.
And don’t even get me started on coiling. You’re just stuffing metal into your skull and hoping it sticks. 15.7% retreatment rate? That’s not a treatment, that’s a subscription service. I’d rather just stop smoking and drink kombucha instead.
Honestly, this post gave me hope. I didn’t realize how much control we actually have. Quitting smoking cut risk by 54%? That’s like getting a free pass to live longer. I’ve been meaning to quit for years - this is my sign. And the PHASES score? It’s not scary if you know the numbers. I’m getting my annual MRA next month. Small aneurysm, low score. No surgery needed. Just better habits. You got this.
Also - if you’re reading this and you smoke? Just one day. One day without a cigarette. You can do it.
Flow diversion requires blood thinners long-term. That’s a dealbreaker for anyone with a history of GI bleeds or falls. Not everyone can handle that. Coiling’s not perfect either. But clipping? Still the gold standard if you’re young and healthy. One size doesn’t fit all.
I’ve got a 4mm aneurysm in my AComm. No symptoms. Never smoked. BP’s perfect. Doc says watch and wait. I’m not stressing. I’m not drinking. I’m sleeping. I’m breathing. That’s my treatment plan. Science says I’m fine. So I’m fine.
Also, the WEB device looks like a tiny metal donut. That’s wild.
Lol. Just don’t smoke. 😎
The fact that we can now predict rupture risk with 72% accuracy using machine learning models analyzing 42 variables… it’s nothing short of miraculous. We’ve moved from guesswork to precision medicine. This isn’t just progress - it’s evolution. The lives saved by these tools will echo through generations. I am humbled.
So we’re told to stop smoking but no one talks about how the whole medical system is built on profit. Who funds these studies? Who profits from coiling vs clipping? Who gets paid when you get a stent? The PHASES score sounds legit but what if it’s just a way to justify more procedures? I mean… think about it. We’re told to trust science but we’re also told to trust corporations. Contradiction much?
Have you ever wondered why the government doesn’t screen everyone for aneurysms? Why it’s not mandatory? Why it’s not covered under Medicare? Because they don’t want you to know how common it is. They want you to panic when it’s too late - then you’ll pay for the procedure. The 3.2% stat? That’s the tip of the iceberg. They don’t want you scanning your own brain. They want you scared… and paying.
It’s fascinating how biology and chance intersect here. Aneurysms form silently, often in places where arteries bend or branch - places of mechanical stress. It’s not just genetics or smoking - it’s physics. Blood flow is a fluid dynamics problem. The body is a pipe system under pressure. And we’re trying to fix it with tiny coils and mesh stents. We’re engineering our own survival. That’s profound. We’re not just treating disease - we’re redesigning biology with titanium and platinum. And yet, the simplest solution remains: breathe. Don’t smoke. Lower your pressure. Let the body heal itself. Sometimes the most elegant solution is the quietest one.
I got my aneurysm checked last year. Score was 2. Low risk. No surgery. But I quit smoking cold turkey after reading this. Also started meditating. Changed my diet. Lost 20 lbs. My BP is now 122/78. This isn’t just about surviving - it’s about living better. If this saves one person, it’s worth it. 🙌
You people act like this is a miracle. It’s not. It’s just medicine. People die from this every day because they ignored symptoms. You don’t get a trophy for not smoking. You get to live. That’s basic.
The fact that women are 1.6 times more likely to have aneurysms and yet research funding is skewed toward male-centric conditions speaks volumes. We treat symptoms like they’re gender-neutral but biology isn’t. And nobody’s talking about it. Just saying.