Impetigo vs Cellulitis: Identifying Skin Infections and Choosing Antibiotics

Imagine waking up with a strange rash that looks like honey-colored crusts on your child's face, or noticing a patch of skin on your leg that's suddenly red, hot, and swollen. While both might seem like simple skin irritations, they could be two very different bacterial invasions: Impetigo is a highly contagious superficial skin infection common in children, often appearing as crusty sores. It typically stays on the surface, but if you're dealing with Cellulitis, you're facing a deeper bacterial infection of the dermis and subcutaneous tissues that can spread rapidly if ignored.
The danger here isn't just the rash; it's picking the wrong treatment. Using a mild cream for a deep-tissue infection or over-prescribing heavy antibiotics for a surface sore doesn't just fail the patient-it feeds the rise of antibiotic-resistant bacteria. Knowing exactly which one you're fighting is the first step toward getting rid of it fast.
Spotting the Difference: Surface vs. Deep
If you aren't a doctor, telling these two apart can be tricky because both involve redness and bacteria. However, the "depth" of the infection is the biggest clue. Impetigo is like a smudge on a window; it's right on the surface. Cellulitis is more like a stain that has soaked through the glass into the wall.
Impetigo usually comes in two flavors. The most common is nonbullous, where you see small red sores that pop and leave behind a distinct honey-colored crust. Then there's bullous impetigo, which features larger, clear-fluid-filled blisters (bullae) that can reach 2-5 cm in size. Because it's so superficial, it spreads like wildfire in schools and daycares, often earning the nickname "school sores."
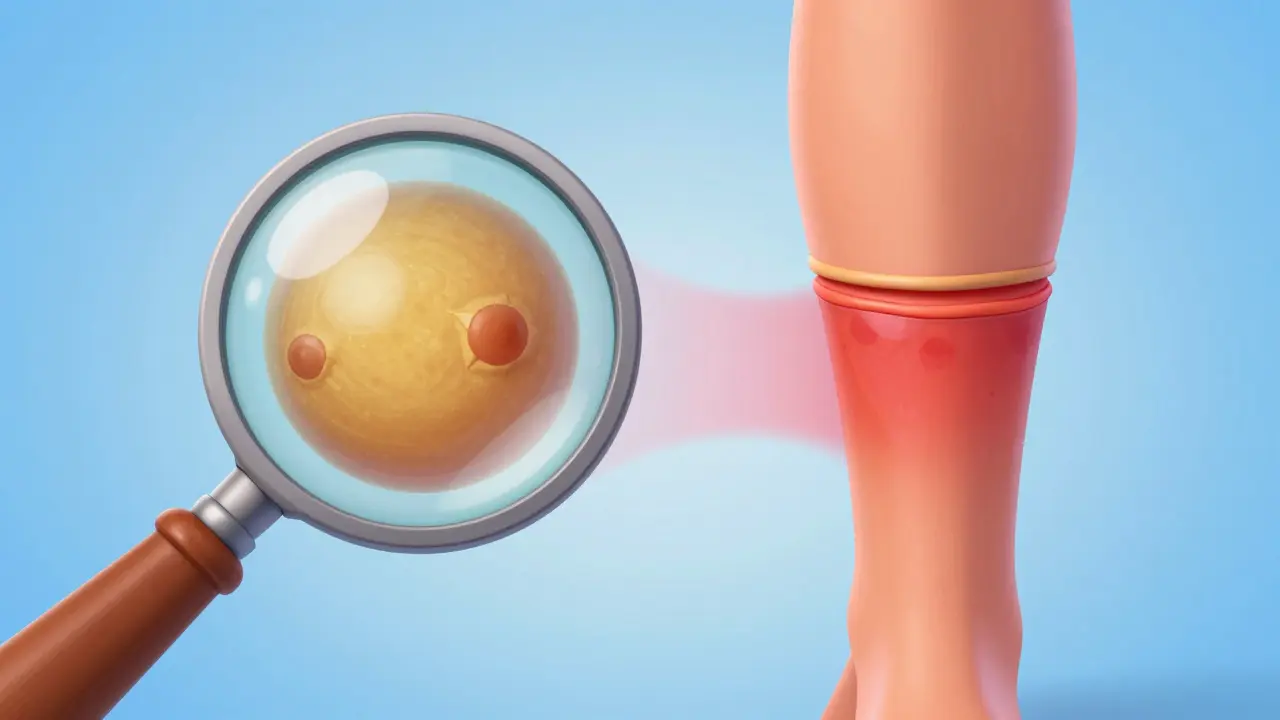
Cellulitis is a different beast. It doesn't usually crust over. Instead, the skin feels tight, warm to the touch, and looks swollen. The borders are often blurry and poorly defined, making it hard to see exactly where the infection ends and healthy skin begins. If you notice the redness is moving up your limb or you start feeling feverish, you're likely dealing with a deeper infection that needs immediate attention to avoid systemic complications like sepsis.
| Feature | Impetigo | Cellulitis |
|---|---|---|
| Depth | Superficial (Epidermis) | Deep (Dermis & Subcutaneous) |
| Key Visual | Honey-colored crusts / Blisters | Diffuse redness, swelling, warmth |
| Common Bacteria | Staphylococcus aureus | Streptococcus species |
| Contagion Risk | Extremely High | Low (not typically contagious) |
| Primary Risk | Spread to others/other skin areas | Sepsis, Toxic Shock Syndrome |
The Usual Suspects: Which Bacteria is Responsible?
Both infections are usually caused by the same couple of bacterial "families," but they prefer different layers of skin. Staphylococcus aureus is the primary driver behind most impetigo cases. It's a hardy bacterium that can sometimes invade even intact skin, though it usually sneaks in through a tiny cut or an insect bite.
On the other hand, Streptococcus is more frequently the culprit in cellulitis. While Staph can also cause deep infections, the classic "spreading redness" of cellulitis is often the calling card of Strep. There is a close relative to cellulitis called erysipelas, which is essentially a superficial version of cellulitis with very sharp, defined borders, almost exclusively caused by Streptococcus.
The real headache for doctors today is MRSA (Methicillin-resistant Staphylococcus aureus). This is a strain of Staph that has learned how to ignore the most common antibiotics. If you have MRSA, the standard pills your doctor might have given you ten years ago simply won't work. This is why some doctors now insist on a culture test-swabbing the infection to see exactly which bug is living there-before prescribing a heavy-duty antibiotic.
Navigating Antibiotic Choices
Choosing the right medication depends heavily on where you live and how severe the infection is. Interestingly, different countries have different "first-choice" drugs based on the resistance patterns they see in their local clinics.
For a mild case of impetigo, you might not even need a pill. A topical cream like mupirocin is often the go-to; it's highly effective (around 90% success rate) for localized sores. However, if the sores are all over the body, oral antibiotics become necessary. In the UK, doctors often reach for flucloxacillin, while in France, amoxicillin-clavulanate or pristinamycin are more common for tougher cases.
Cellulitis is a more serious matter and almost always requires oral antibiotics for 5 to 14 days. Again, the choice varies: the UK favors flucloxacillin, while French guidelines lean toward amoxicillin. If the bacteria is suspected to be MRSA, doctors have to pivot to stronger agents like vancomycin or clindamycin. If you start showing systemic symptoms-like a high fever, chills, or the infection isn't responding to pills-hospitalization for IV antibiotics is often the only safe route.

Practical Steps for Recovery and Prevention
Antibiotics do the heavy lifting, but your home care determines how quickly you bounce back and whether the infection returns. For those with recurrent cellulitis, especially people with diabetes or venous insufficiency, a single episode often leads to another if the underlying cause isn't managed.
If you're managing impetigo at home, especially with kids, follow these rules to stop the spread:
- The 24-Hour Rule: Children should usually stay home from school or daycare until they have been on antibiotics for at least 24 hours.
- Don't Share: Towels, washcloths, and clothing should be strictly personal. Once used on an infected area, wash them in hot water immediately.
- Keep it Clean: Gently wash the sores with soap and water. Avoid scrubbing, which can damage the skin and push bacteria deeper.
- Seal the Breach: Use a clean bandage to cover sores, preventing the bacteria from hitching a ride to other parts of the body or other people.
For cellulitis, the focus is on reducing swelling. Elevating the affected limb (like a leg or arm) helps the fluid drain and speeds up the healing process. It's also vital to complete the entire course of antibiotics, even if the redness disappears after three days. Stopping early is a fast track to a relapse or, worse, creating a drug-resistant strain of bacteria in your own body.
When to Panic (and When to Wait)
Most skin infections are manageable, but some turn deadly quickly. The window for optimal treatment is generally 48 to 72 hours. If you wait a week to see a doctor, you're significantly increasing the risk of the infection hitting your bloodstream.
You need to head to the emergency room if you notice any of the following "red flags":
- Rapid Progression: The redness is spreading visibly by the hour.
- Systemic Sickness: You have a high fever, shaking chills, or feel suddenly confused.
- Skin Changes: The area becomes purple, black, or develops blisters (this can indicate a much more severe necrosis).
- Pain Disproportion: The area hurts way more than it looks like it should, which can be a sign of a deeper, more aggressive infection.
Can impetigo be cured without antibiotics?
While very mild cases of impetigo might resolve with careful cleaning and hygiene, it is highly contagious and can spread rapidly. Antibiotics-either topical creams like mupirocin or oral medications-are strongly recommended to clear the infection and prevent it from spreading to other people or deeper into the skin.
Is cellulitis contagious?
Generally, no. Cellulitis is an infection of the deep layers of the skin. Unlike impetigo, you cannot "catch" cellulitis simply by touching someone's affected skin. However, the bacteria that cause it (like Streptococcus) can be present on the skin; the infection only happens when those bacteria find a way into the deeper tissue through a cut, bite, or surgical wound.
How long does it take for cellulitis to clear up?
Most uncomplicated cases of cellulitis resolve within 7 to 14 days of consistent antibiotic treatment. Some patients may notice the redness fading quickly, but the full course of medication must be completed to ensure the bacteria are entirely eliminated from the deeper tissues.
Why do I keep getting cellulitis in the same spot?
Recurrent cellulitis often happens because the skin barrier in that area is permanently compromised. Common causes include chronic venous insufficiency (poor circulation in the legs), lymphedema, or uncontrolled diabetes. If you have recurring infections, you should investigate these underlying health issues with a doctor to prevent permanent tissue damage.
What is the difference between a rash and cellulitis?
A typical rash is often an allergic reaction or irritation and is usually itchy. Cellulitis is an infection; it typically feels hot, painful, and swollen. If the red area is expanding and you feel unwell, it is likely an infection rather than a simple rash. Because misdiagnosis can lead to sepsis, any "rash" accompanied by warmth and swelling should be evaluated by a professional.